Duchenne Muscular Dystrophy (DMD)
About Duchenne
Duchenne Muscular Dystrophy (DMD) is a paediatric neuromuscular disorder predominantly affecting the male children. Dystrophin is a muscle protein which helps the muscle cells maintain their basic shape, integrity and strength. The absence or the low levels of this protein production leads to muscle breakdown, gradually rendering the person weak. This disease is rapidly progressive and the incidence is approximately 1 in 3500 live male births in the world. The onset of DMD is characterized by muscle loss at the pelvic region, then in the upper arms and finally it takes a toll on the heart and lung muscles, leading to death ultimately.
We Offer Following Services For Duchenne Muscular Dystrophy
1. Diagnostics
2. Counseling
3. Multidisciplinary Care
4. Physiotherapy
5. Family support
6. Outreach
Inheritance of DMD
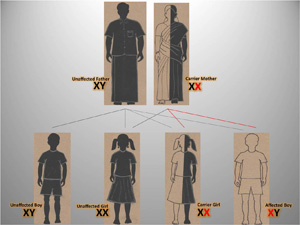
The Dystrophin gene is present only on the X chromosome. Thus, the inheritance of DMD is through the X chromosome. Due to the presence of only one X chromosome in males, the defective gene’s function cannot be compensated. This in turn affects the production of dystrophin protein resulting in abnormal nerve-muscle coordination. In females, on the other hand, due to the presence of two X chromosomes, one can compensate for the other X chromosome’s mutated genes. Females, thus do not show any symptoms and become carriers of the disorder. The sons of females (carriers) will have a 50% chance of inheriting the disease. While, each of the daughter have a 50% chance of being ending up as carriers.
Symptoms of DMD
Symptoms usually appear before the age of 6. There is a steady decline in the muscle strength between the ages of 6 to 11. By age 10, crutches may be required for walking and by age of 12 most boys use a wheelchair. The following are the most noticeable and distinguishing symptoms of DMD:
Delay In Attaining Motor Milestones
1. Difficulty in sitting and standing
2. Delay in walking- Mean age of walking for DMD boys is 18 months whereas for normal children, the mean age is 12 months.
Muscle Weakness And Deterioration
1. Progressive weakening of legs and pelvic muscle
2. Frequent falls
3. Waddling gait
4. Difficulty in climbing stairs
5. Muscle weakness also seen in arms, neck and other areas
6. Gower’s sign- Difficulty in getting up from sitting to standing position
7. Respiratory and cardiac difficulties (Late teens and early twenties)
8. Enlargement of calf muscles due to fat accumulation (Pseudohypertrophy)
Diagnosis
Biochemical Identification
Blood test to measure Serum Creatine Kinase: Serum creatine kinase is an enzyme present in the muscle whose levels are abnormally elevated in the serum of the patients (10 x 100 times normal concentration) affected.
Genetic
The methods currently being used are multiplex Polymerase Chain Reaction (mPCR), Multiplex Ligation Probe Amplification (MLPA) and sequencing. Together, these methods can confirm the disorder in about 98% of the cases.
Muscle Biopsy
A muscle biopsy can be used to differentiate between different types of muscular dystrophy using immunohistochemistry. The dystrophin protein can be visualized by staining the muscle sample with a special dye. A boy with Duchenne, will have an absence of dystrophin. Some individuals can be found to have a lower amount of the dystrophin protein, classified as having Becker muscular dystrophy.
Treatment and Cure – The Future of Duchenne
Till date, there is no known cure for DMD. Presently, treatment aims to control symptoms to maximize quality of life. Gene therapy that targets the Duchenne gene may become available in the future. Some scientists are trying to fix the defective genes so that they will make the dystrophin protein in the right quantity. Others are trying to make the chemicals that will mimic the proteins in the body. This will lead to treatment that will halt the progression of the disease.
As mentioned before, current treatment is designed to prevent or reduce the symptoms as much as possible. For example, there are treatments to reduce deformities in joints and the spine so that people can remain mobile, for as long as possible. Respiratory therapy and physical therapy are considered to prevent painful muscle contractures, orthopedic appliances are used for support and corrective orthopedic surgery may be needed to improve the quality of life. As we rely on muscles to breathe, some children with DMD need respiratory aids, such as a ventilator, to help them breathe. Cardiac abnormalities may require a pacemaker. For some types of Muscular Dystrophy (MD), medication can help. Corticosteroids such as prednisone and Deflazacort can slow the rate of muscle deterioration in patients with DMD but causes side effects.
There are things that children with MD can do to help their muscles. Certain exercises and physical therapy can help them avoid contractures, a stiffening of the muscles near the joints that can make it harder to move and can lock the joints in painful positions. Often, teens are fitted with special braces to ensure flexible joints and tendons (the strong, rubber band-like tissues that attach muscles to bones). Surgery is sometimes used to reduce pain and increase movement from contractures. Clinicians are also dedicated to finding the best ways to treat the symptoms of MD so that children, teens and adults with the disease can live as comfortably and happily as possible.
Importance of Carrier Analysis for Prevention
Advances in molecular studies have allowed the characterization of mutations responsible for DMD and the accurate identification of female carriers, as well as prenatal diagnosis. Identification of carriers of DMD is an important aspect of prevention in families in which this disease is present. In addition a number of affected males, probably as many as a third of the total, will be born to normal, non-carrier females and differentiation of these is essential for accurate counseling.
The first essential step in genetic counseling is to verify the diagnosis in the index case. Next, a detailed family tree is to be constructed before investigation of the possible carrier is begun. Practically, if the mother of an affected boy (proband) has another affected relative, she must be an obligate carrier. If there is an affected brother or at least one affected son, she is a possible carrier. But in most families there is only one affected patient. Therefore, female relatives of affected males are candidates for carrier assessment. Since carriers are asymptomatic, genetic tests are used to confirm their carrier status.
Once carrier status is established, the relative is referred to a genetic counselor who will advise them on the risk of having a child with DMD during their next pregnancy. Carrier analysis is the best methods for the prevention of DMD today.